
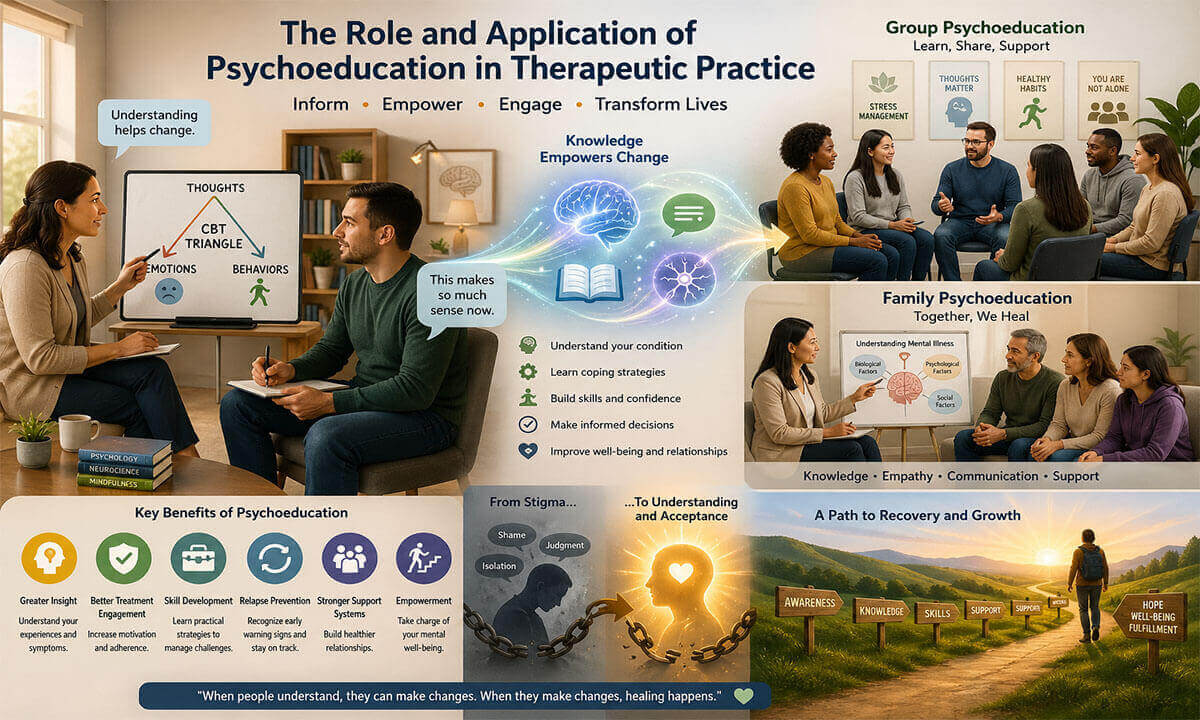
The Role and Application of Psychoeducation in Therapeutic Practice:
Psychoeducation has become a foundational component of modern therapeutic practice, bridging the gap between clinical knowledge and clients’ lived experiences. At its core, psychoeducation involves providing individuals and their families with structured, evidence-based information about mental health conditions, treatment options, coping strategies, and recovery processes. Rather than positioning clients as passive recipients of care, psychoeducation aligns with collaborative and client-centered approaches, empowering individuals to understand and actively participate in their own healing journey (Swift & Parkin, 2017). Over the past several decades, psychoeducation has evolved from a supplementary tool to an integral therapeutic intervention across a wide range of psychological disorders, including addiction, schizophrenia, bipolar disorder, anxiety, depression, and attention-deficit/hyperactivity disorder (ADHD). Its applications extend across individual, group, and family therapy settings, often enhancing treatment adherence, improving outcomes, and reducing relapse rates. In the rest of this article, we will explore the role and application of psychoeducation in therapeutic practice.
Conceptual Foundations of Psychoeducation:
The conceptual foundations of psychoeducation lie at the intersection of cognitive, behavioral, neurobiological, and humanistic traditions in psychology. At its essence, psychoeducation is built on a simple yet powerful premise: understanding fosters change. When individuals gain accurate, meaningful knowledge about their psychological experiences, they are better equipped to interpret symptoms, regulate emotions, and engage in adaptive behaviors. However, psychoeducation is not merely the passive transmission of information; it is an active, collaborative, and context-sensitive process that integrates scientific knowledge with personal meaning-making.
- Knowledge as a Therapeutic Agent: One of the central assumptions underlying psychoeducation is that knowledge itself can function as a therapeutic tool. Psychological distress is often maintained or intensified by misunderstanding, misinformation, or maladaptive beliefs. For example, individuals experiencing anxiety may misinterpret physiological arousal as dangerous, while those with depression may view their condition as a personal failure rather than a treatable disorder. Psychoeducation addresses these distortions by providing clear, evidence-based explanations that reframe experiences in a more accurate and less threatening way.
From a cognitive perspective, this process aligns with principles of cognitive restructuring, where inaccurate beliefs are identified and replaced with more adaptive interpretations. By learning about symptom mechanisms (such as the role of negative automatic thoughts in depression or the fight-or-flight response in anxiety), clients begin to reinterpret their internal experiences, reducing fear and increasing perceived control.
- Integration of Neuroscientific Understanding: Contemporary psychoeducation increasingly incorporates insights from neuroscience to deepen clients’ understanding of mental processes. Explaining how brain systems regulate emotion, motivation, and decision-making can demystify complex behaviors and reduce self-blame. For instance, neuroscience-informed psychoeducation in addiction highlights how alterations in reward circuitry and impulse control contribute to substance use patterns, helping individuals see addiction as a brain-based condition rather than a moral failing (Ekhtiari et al., 2017).
This neurobiological framing serves multiple functions: it enhances credibility, normalizes experiences, and provides a concrete foundation for behavior change. When clients understand that their difficulties have identifiable biological components, they may become more open to treatment and more compassionate toward themselves.
- Client-Centered and Collaborative Orientation: A defining feature of psychoeducation is its alignment with client-centered therapy principles. Rather than positioning the therapist as the sole expert, psychoeducation acknowledges the client’s lived experience as an essential source of knowledge. This perspective reflects the broader shift in psychotherapy toward collaboration and shared decision-making. Clients are encouraged to question, interpret, and apply information in ways that are personally meaningful, reinforcing their role as active participants in the therapeutic process (Swift & Parkin, 2017).
This collaborative stance also enhances therapeutic alliance, which is a key predictor of positive outcomes. When clients feel respected and involved, they are more likely to engage with the material and integrate it into their daily lives.
- Learning Theory and Skill Acquisition: Psychoeducation is deeply rooted in principles of learning theory, particularly social learning and behavioral models. It is not limited to imparting knowledge but also aims to facilitate skill acquisition. Clients learn practical strategies (such as emotion regulation techniques, problem-solving skills, and coping mechanisms) that can be applied in real-world contexts.
This educational component often follows a structured format, including explanation, modeling, rehearsal, and feedback. For example, in stress management programs, clients may first learn about the physiological effects of stress, then practice relaxation techniques, and finally apply these skills in their daily routines. Such integration of knowledge and action ensures that psychoeducation translates into meaningful behavioral change.
- Normalization and Reduction of Stigma: Another vital conceptual pillar of psychoeducation is normalization. Many individuals experiencing psychological difficulties feel isolated, confused, or ashamed. By providing information about the prevalence, causes, and course of mental health conditions, psychoeducation helps normalize these experiences. Clients come to understand that their struggles are not unique or indicative of personal weakness but are part of broader, well-documented patterns.
This normalization process plays a vital role in reducing stigma; both societal and self-directed. When individuals reframe their experiences through an informed lens, they are less likely to internalize negative stereotypes and more likely to seek and adhere to treatment.
- Empowerment and Self-Efficacy: Psychoeducation is fundamentally empowering. It equips individuals with the knowledge and tools needed to make informed decisions about their treatment and well-being. This aligns with the concept of self-efficacy; the belief in one’s ability to manage challenges and achieve desired outcomes. As clients gain understanding and develop skills, their confidence in managing symptoms increases, leading to greater autonomy and resilience.
Empowerment is particularly important in chronic conditions, where long-term self-management is essential. By teaching clients how to recognize early warning signs, implement coping strategies, and navigate setbacks, psychoeducation fosters a sense of control and preparedness.
- Social and Systemic Dimensions: Beyond the individual level, psychoeducation also has important social and systemic dimensions. In family and group settings, it facilitates shared understanding and improves communication. Family members who are educated about a loved one’s condition are better able to provide support, manage expectations, and reduce interpersonal conflict. This systemic approach recognizes that mental health is influenced by relational and environmental factors, and that education can create more supportive contexts for recovery.
Key Roles of Psychoeducation in Therapy:
Psychoeducation serves multiple, interrelated roles within therapeutic practice, extending far beyond the simple provision of information. It functions as a catalyst for insight, a motivator for engagement, and a foundation for behavioral and emotional change. When effectively integrated into therapy, psychoeducation enhances both the process and outcomes of treatment by equipping clients with the knowledge, skills, and confidence needed to navigate their psychological challenges. Here we explore its key roles.
1. Enhancing Insight and Self-Awareness: One of the most fundamental roles of psychoeducation is to foster insight into the nature of psychological difficulties. Many clients enter therapy with limited or distorted understandings of their symptoms, often attributing them to personal weakness, moral failure, or external circumstances beyond their control. Psychoeducation helps reframe these interpretations by providing scientifically grounded explanations of mental health conditions.
For example, individuals with anxiety may learn about the physiological basis of the fight-or-flight response, while those with depression may gain insight into the interaction between cognition, emotion, and behavior. In addiction contexts, neuroscience-informed psychoeducation explains how brain reward systems and impaired executive functioning contribute to substance use patterns (Ekhtiari et al., 2017). This type of understanding reduces confusion and fear, allowing clients to view their experiences more objectively.
Pointedly, increased insight is not purely intellectual; it has emotional consequences. As clients begin to understand why they feel and behave in certain ways, they often experience relief, reduced self-blame, and greater self-compassion. This shift creates a more constructive internal environment for therapeutic change.
2. Promoting Treatment Engagement and Adherence: Psychoeducation plays an essential role in enhancing clients’ engagement with therapy and adherence to treatment recommendations. When individuals understand the rationale behind specific interventions (whether pharmacological or psychotherapeutic), they are more likely to perceive them as credible and beneficial.
For instance, explaining how antidepressant medications influence neurotransmitter systems or how cognitive-behavioral techniques target maladaptive thought patterns can demystify treatment processes. This understanding reduces resistance, addresses misconceptions, and fosters trust in the therapeutic approach. Research indicates that psychoeducation significantly improves treatment compliance, particularly in long-term conditions where sustained engagement is essential (Unterecker, 2019).
Moreover, psychoeducation helps align expectations between the therapist and client. By clarifying the goals, structure, and potential challenges of therapy, it prepares clients for the work involved and reduces the likelihood of premature dropout.
3. Supporting Behavioral Change and Skill Development: Another central role of psychoeducation is to facilitate the development of practical skills that enable clients to manage their symptoms effectively. Knowledge alone is insufficient for change; it must be paired with actionable strategies that clients can apply in their daily lives.
Psychoeducational interventions often include training in coping mechanisms such as stress management, emotion regulation, problem-solving, and communication skills. For example, large-group psychoeducation programs for anxiety and depression teach participants how to identify stressors, challenge negative thoughts, and implement relaxation techniques. These interventions have been shown to produce significant improvements in symptom severity and overall functioning (Dolan et al., 2021).
This role is closely linked to learning theory, as psychoeducation typically involves a structured process of instruction, modeling, practice, and feedback. Through repeated application, clients internalize these skills, leading to sustainable behavioral change.
4. Reducing Relapse and Supporting Long-Term Management: Psychoeducation is particularly valuable in the management of chronic and recurrent mental health conditions. It equips clients with the tools needed to recognize early warning signs, anticipate challenges, and implement preventive strategies.
In disorders such as bipolar disorder and schizophrenia, relapse prevention is a key treatment goal. Psychoeducational programs teach clients to monitor mood fluctuations, identify triggers, and adhere to treatment plans. Evidence from randomized controlled trials suggests that psychoeducation can be as effective as cognitive-behavioral therapy in reducing relapse rates in bipolar disorder (Parikh et al., 2012).
By fostering a proactive approach to mental health, psychoeducation shifts the focus from crisis intervention to ongoing self-management. Clients become better prepared to handle setbacks, reducing the severity and duration of future episodes.
5. Normalizing Experiences and Reducing Stigma: A powerful yet often underestimated role of psychoeducation is its ability to normalize psychological experiences. Many individuals feel isolated or ashamed of their symptoms, believing that they are alone in their struggles. Psychoeducation counters this by providing information about the prevalence and commonality of mental health conditions.
This normalization reduces both internalized stigma and societal stigma. Clients begin to understand that their experiences are part of broader, well-recognized patterns rather than signs of personal inadequacy. As a result, they may feel more comfortable discussing their difficulties, seeking support, and engaging in treatment.
Normalization also extends to emotional responses. By learning that reactions such as fear, sadness, or anger are understandable given their circumstances, clients can develop greater emotional acceptance and resilience.
6. Strengthening Therapeutic Alliance: The therapeutic relationship is a cornerstone of effective therapy, and psychoeducation contributes significantly to its development. By sharing knowledge in a transparent and collaborative manner, therapists demonstrate respect for clients’ capacity to understand and participate in their treatment.
This process fosters trust, openness, and mutual understanding. Clients who feel informed and involved are more likely to view the therapist as a partner rather than an authority figure. This aligns with the perspective that clients are “experts” in their own experiences, and that therapy should be a collaborative endeavor (Swift & Parkin, 2017).
A strong therapeutic alliance not only enhances engagement but also serves as a protective factor against dropout and poor outcomes.
7. Enhancing Family and Social Support Systems: Psychoeducation often extends beyond the individual to include family members and significant others. In many cases, the social environment plays a crucial role in the development and maintenance of psychological difficulties. Educating family members about a client’s condition can improve communication, reduce conflict, and foster a more supportive atmosphere.
For example, family psychoeducation in schizophrenia has been shown to reduce relapse rates and improve overall functioning by helping relatives understand the nature of the disorder and develop effective coping strategies (Anderson et al., 1980). This systemic approach recognizes that recovery is not solely an individual process but is influenced by interpersonal dynamics.
8. Facilitating Motivation and Readiness for Change: Finally, psychoeducation supports motivation by helping clients understand the consequences of their behaviors and the benefits of change. This is particularly important in conditions where ambivalence is common, such as addiction.
By increasing awareness and providing a clear rationale for change, psychoeducation complements motivational approaches like motivational interviewing. It helps clients move through stages of change by enhancing their readiness and commitment to treatment (Hettema et al., 2005).
Applications Across Clinical Contexts:
Psychoeducation is a highly adaptable intervention that can be applied across diverse clinical populations, therapeutic modalities, and treatment settings. Its flexibility allows it to be tailored to the specific needs of individuals, families, and groups, as well as to the characteristics of different psychological disorders. Rather than functioning as a one-size-fits-all approach, psychoeducation is most effective when it is context-sensitive; integrated with other therapeutic techniques and aligned with the developmental, cultural, and clinical profiles of the target population. Here we examine its applications across key clinical contexts.
1. Family-Based Psychoeducation in Severe Mental Illness: One of the earliest and most influential applications of psychoeducation has been in family-based interventions for severe mental illnesses, particularly schizophrenia. In such contexts, psychoeducation extends beyond the individual to include family members, recognizing that the social environment plays a critical role in both the course and management of the disorder.
Family psychoeducation programs typically provide information about the nature, symptoms, and course of schizophrenia, as well as guidance on communication skills, problem-solving, and relapse prevention strategies. By helping family members understand the biological and psychological underpinnings of the illness, these interventions reduce blame, guilt, and unrealistic expectations.
Seminal work by Anderson et al. (1980) demonstrated that psychoeducational family interventions significantly reduce relapse rates and improve functional outcomes. This effect is largely attributed to reductions in “expressed emotion” (e.g., criticism, hostility), which has been strongly linked to relapse in schizophrenia. Moreover, families become better equipped to support treatment adherence and recognize early warning signs of relapse, contributing to more stable long-term outcomes.
2. Group Psychoeducation for Common Mental Disorders: Group-based psychoeducation has become a widely used and cost-effective approach for treating common mental health conditions such as anxiety and depression. These programs are often delivered in structured formats, such as workshops or multi-session courses, and combine educational content with practical exercises.
In large-group psychoeducation for stress, anxiety, and depression, participants learn about the cognitive, emotional, and physiological components of these conditions. They are also introduced to coping strategies such as relaxation techniques, cognitive restructuring, and behavioral activation. The group setting offers additional benefits, including peer support, normalization of experiences, and opportunities for shared learning.
A systematic review and meta-analysis by Dolan et al. (2021) found that large-group psychoeducation interventions are effective in reducing symptoms of anxiety and depression, with outcomes comparable to more intensive individual therapies in some cases. This makes group psychoeducation particularly valuable in settings with limited resources, such as community mental health services or educational institutions.
3. Psychoeducation in Neurodevelopmental Disorders (e.g., ADHD): Psychoeducation plays a crucial role in the management of neurodevelopmental disorders such as attention-deficit/hyperactivity disorder (ADHD), particularly among children and adolescents. In these contexts, psychoeducation is often directed at both the individual and their caregivers, including parents and teachers.
For young people with ADHD, psychoeducation helps them understand their attentional difficulties, impulsivity, and hyperactivity in a non-stigmatizing way. This understanding can improve self-esteem and reduce frustration. For caregivers, psychoeducation provides strategies for behavior management, communication, and academic support.
Meta-analytic evidence indicates that psychoeducational interventions significantly improve social skills and overall functioning in young people with ADHD (Powell et al., 2021). By fostering a shared understanding among all stakeholders, psychoeducation creates a more supportive and structured environment, which is essential for effective intervention.
4. Integration with Mindfulness and Contemporary Therapeutic Approaches: In recent years, psychoeducation has been increasingly integrated with contemporary therapeutic modalities, such as mindfulness-based interventions. This integration reflects a shift toward more holistic approaches that address both cognitive understanding and experiential learning.
For example, mindfulness-based psychoeducation programs for early-stage schizophrenia combine traditional educational components with mindfulness practices that enhance present-moment awareness and emotional regulation. Participants not only learn about their condition but also develop skills to observe their thoughts and feelings without judgment.
An 18-month randomized controlled trial by Chien et al. (2019) demonstrated that such integrated programs lead to sustained improvements in symptom management, functioning, and quality of life. This suggests that combining psychoeducation with experiential techniques can enhance its effectiveness by addressing both intellectual and emotional aspects of psychological functioning.
5. Psychoeducation in Mood Disorders (e.g., Bipolar Disorder): Psychoeducation is a cornerstone of treatment for mood disorders, particularly bipolar disorder, where relapse prevention and long-term management are critical. In this context, psychoeducation focuses on helping individuals understand the cyclical nature of mood episodes, identify triggers, and maintain treatment adherence.
Structured psychoeducational programs often include information about sleep regulation, medication management, stress reduction, and early warning signs of manic or depressive episodes. Clients are encouraged to monitor their mood and behavior patterns, fostering a proactive approach to managing their condition.
Research by Parikh et al. (2012) found that psychoeducation is as effective as cognitive-behavioral therapy in improving outcomes for individuals with bipolar disorder. This highlights its value as both a standalone and adjunctive intervention, particularly in long-term care.
6. Psychoeducation in Addiction Treatment: In addiction treatment, psychoeducation is used to increase awareness of the biological, psychological, and social factors that contribute to substance use. Neuroscience-informed psychoeducation, in particular, helps individuals understand how changes in brain structure and function influence craving, decision-making, and relapse.
By framing addiction as a chronic, brain-based condition, psychoeducation reduces stigma and promotes a more compassionate self-view. It also supports the development of coping strategies for managing triggers and high-risk situations.
Psychoeducation is often integrated with motivational interviewing and relapse prevention strategies, enhancing clients’ readiness for change and commitment to recovery (Hettema et al., 2005; Ekhtiari et al., 2017). This combination is especially effective in addressing ambivalence and fostering sustained behavioral change.
7. Psychoeducation in Pharmacological Treatment and Compliance: Another important application of psychoeducation is in supporting pharmacological treatment. Many clients have concerns or misconceptions about psychiatric medications, which can lead to poor adherence and suboptimal outcomes.
Psychoeducation addresses these issues by providing clear information about how medications work, their potential side effects, and the importance of consistent use. This transparency helps build trust and reduces anxiety about treatment.
Unterecker (2019) emphasizes that psychoeducation significantly improves medication compliance, particularly in chronic conditions where long-term treatment is required. By involving clients in decision-making and addressing their concerns, psychoeducation fosters a sense of ownership and responsibility for treatment.
8. Community and Preventive Mental Health Settings: Beyond clinical settings, psychoeducation is increasingly used in community and preventive mental health initiatives. Schools, workplaces, and public health programs often incorporate psychoeducational components to promote mental health awareness, reduce stigma, and encourage early intervention.
In these contexts, psychoeducation may focus on topics such as stress management, emotional resilience, and recognizing early signs of mental health difficulties. By reaching individuals before problems become severe, these programs contribute to prevention and early treatment, ultimately reducing the burden on healthcare systems.
Mechanisms Underlying Effectiveness:
The effectiveness of psychoeducation in therapeutic practice is not incidental; rather, it is driven by a set of well-established psychological, cognitive, and social mechanisms that work together to facilitate meaningful and sustained change. These mechanisms explain how and why psychoeducation leads to improvements in insight, behavior, emotional regulation, and overall functioning. Understanding these underlying processes is essential for clinicians, as it allows them to apply psychoeducation more strategically and tailor it to individual client needs.
1. Cognitive Restructuring and Meaning-Making: One of the primary mechanisms through which psychoeducation exerts its impact is cognitive restructuring. Many psychological difficulties are maintained by maladaptive beliefs, misinterpretations, and cognitive distortions. Psychoeducation introduces accurate, evidence-based information that challenges these distortions and replaces them with more adaptive interpretations.
For instance, a client with panic disorder may initially interpret a rapid heartbeat as a sign of imminent danger. Through psychoeducation, they learn that this response is part of the body’s natural fight-or-flight system. This reinterpretation reduces catastrophic thinking and associated anxiety. In this way, psychoeducation facilitates a shift from threat-based appraisal to informed understanding.
Beyond correcting misinformation, psychoeducation also supports meaning-making. Clients begin to construct coherent narratives about their experiences, integrating symptoms into a broader psychological and biological framework. This process enhances a sense of clarity and reduces the chaos often associated with mental distress.
2. Emotional Normalization and Regulation: Psychoeducation plays a critical role in normalizing emotional experiences. Many clients perceive their emotional reactions as abnormal, overwhelming, or unacceptable, which can intensify distress. By learning that such responses are common and understandable, clients experience a reduction in fear, shame, and self-criticism.
This normalization process is closely linked to emotional regulation. When individuals understand the origins and functions of their emotions, they are better able to manage them. For example, recognizing that anxiety serves a protective function can reduce resistance to the emotion and facilitate more adaptive coping strategies.
Additionally, psychoeducation often includes teaching specific emotion regulation techniques, such as relaxation, mindfulness, or cognitive reframing. These skills provide clients with practical tools to modulate emotional intensity, leading to improved psychological stability.
3. Enhancement of Self-Efficacy and Perceived Control: A central mechanism underlying the success of psychoeducation is the enhancement of self-efficacy; the belief in one’s ability to manage challenges effectively. Psychological distress is frequently accompanied by feelings of helplessness and loss of control. Psychoeducation counteracts these feelings by equipping clients with knowledge and actionable strategies.
As clients learn about their condition and acquire coping skills, they begin to perceive themselves as capable of influencing their own well-being. This increased sense of control is crucial for motivation and persistence in treatment. It encourages active engagement, experimentation with new behaviors, and resilience in the face of setbacks.
Over time, repeated experiences of successfully managing symptoms reinforce self-efficacy, creating a positive feedback loop that supports long-term recovery.
4. Behavioral Activation and Skill Acquisition: Psychoeducation is not limited to cognitive and emotional domains; it also drives behavioral change through skill acquisition and activation. By teaching clients specific strategies (such as problem-solving, communication skills, or stress management), psychoeducation provides the tools necessary for adaptive functioning.
This mechanism is rooted in learning theory, particularly the principles of modeling, rehearsal, and reinforcement. Clients are not only informed about what to do but are often guided through the process of practicing these behaviors in structured ways. For example, in stress management programs, clients may learn relaxation techniques and then apply them in real-life situations.
Behavioral activation is particularly important in conditions like depression, where inactivity and withdrawal perpetuate symptoms. Psychoeducation encourages clients to engage in meaningful activities, thereby interrupting negative behavioral cycles and promoting positive reinforcement.
5. Reduction of Stigma and Self-Stigmatization: Stigma (both societal and internalized) represents a significant barrier to mental health recovery. Psychoeducation addresses this barrier by reframing mental health conditions as understandable and treatable phenomena rather than signs of personal weakness.
By providing information about the prevalence, causes, and course of psychological disorders, psychoeducation reduces feelings of isolation and shame. Clients begin to see their experiences as part of a broader human context, which fosters acceptance and openness.
Reducing self-stigma has important downstream effects, including increased willingness to seek help, greater adherence to treatment, and improved self-esteem. It also enhances interpersonal relationships, as clients may feel more comfortable discussing their experiences with others.
6. Strengthening of Therapeutic Alliance: The therapeutic alliance (the collaborative and trusting relationship between therapist and client) is a key predictor of treatment outcomes. Psychoeducation contributes to this alliance by promoting transparency, collaboration, and mutual understanding.
When therapists share knowledge openly and invite clients to engage with the material, they signal respect for the client’s capacity to understand and contribute to the therapeutic process. This aligns with client-centered approaches that emphasize shared decision-making and empowerment (Swift & Parkin, 2017).
A strong therapeutic alliance enhances engagement, reduces dropout rates, and creates a safe environment for exploration and change. Psychoeducation, by fostering this alliance, indirectly amplifies the effectiveness of other therapeutic interventions.
7. Social Learning and Interpersonal Influence: In group and family settings, psychoeducation operates through mechanisms of social learning and interpersonal influence. Clients observe others with similar experiences, learn from their coping strategies, and receive feedback and support.
This shared learning environment reinforces new behaviors and beliefs, making them more likely to be adopted and maintained. Additionally, family psychoeducation improves communication patterns and reduces conflict, creating a more supportive environment for recovery.
The social dimension of psychoeducation also contributes to normalization, as individuals recognize that they are not alone in their struggles. This sense of belonging can be a powerful motivator for change.
8. Motivational Enhancement and Readiness for Change: Psychoeducation enhances motivation by increasing awareness of the consequences of behaviors and the benefits of change. This is particularly relevant in conditions characterized by ambivalence, such as addiction.
By providing clear, evidence-based information, psychoeducation helps clients evaluate their current behaviors and consider alternative paths. It supports movement through stages of change (from precontemplation to action) by fostering insight and readiness.
When combined with approaches such as motivational interviewing, psychoeducation becomes even more effective in promoting sustained behavioral change, as it aligns knowledge with intrinsic motivation.
Challenges and Considerations:
Despite its well-established benefits, psychoeducation is not a universally effective or inherently sufficient intervention. Its impact depends heavily on how, when, and to whom it is delivered. Without careful consideration of individual, cultural, and contextual factors, psychoeducation can become superficial, overwhelming, or even counterproductive. Therefore, understanding its limitations and the challenges associated with its implementation is essential for maximizing its therapeutic value.
1. Risk of Information Overload: One of the most common challenges in psychoeducation is the tendency to provide excessive or overly complex information. Clients entering therapy are often already experiencing cognitive and emotional strain, which can limit their capacity to absorb and process new material. Presenting large amounts of technical or abstract information in a short time may lead to confusion, disengagement, or even increased anxiety.
Effective psychoeducation requires pacing and prioritization. Clinicians must carefully select what information is most relevant at a given stage of therapy and present it in a clear, digestible manner. Using simple language, visual aids, and repetition can enhance comprehension and retention. Importantly, psychoeducation should be viewed as an ongoing process rather than a one-time event.
2. Lack of Personalization: Psychoeducation is most effective when it is tailored to the individual’s specific needs, experiences, and level of understanding. A standardized, “one-size-fits-all” approach risks failing to resonate with clients or address their unique concerns. For example, two individuals with the same diagnosis may have very different symptom patterns, coping styles, and personal meanings attached to their experiences.
Without personalization, psychoeducation may feel irrelevant or disconnected, reducing engagement and limiting its impact. Clinicians must adapt content based on factors such as age, educational background, cultural context, and readiness for change. Incorporating clients’ personal narratives and encouraging reflection can help bridge the gap between general knowledge and lived experience.
3. Cultural Sensitivity and Contextual Relevance: Cultural beliefs and values play a significant role in how individuals understand and respond to mental health information. Psychoeducational content that is grounded solely in Western biomedical models may not align with the perspectives of clients from diverse cultural backgrounds. This mismatch can lead to misunderstanding, resistance, or rejection of the information.
For instance, some cultures may interpret psychological distress in spiritual or social terms rather than biological ones. In such cases, rigidly imposing a medicalized explanation may undermine therapeutic rapport. Culturally sensitive psychoeducation involves integrating culturally relevant frameworks, respecting clients’ belief systems, and using language and examples that resonate with their context.
4. Timing and Readiness for Information: The effectiveness of psychoeducation is closely tied to the client’s readiness to receive and engage with information. Clients in acute distress, crisis situations, or early stages of therapy may not be emotionally or cognitively prepared to process detailed explanations about their condition.
Providing information prematurely can feel overwhelming or invalidating, particularly if the client is seeking immediate emotional support. Clinicians must assess readiness and introduce psychoeducation gradually, aligning it with the client’s stage of change. In some cases, emotional stabilization and rapport-building may need to precede educational interventions.
5. Overemphasis on Information at the Expense of Experience: While knowledge is a powerful tool, it is not sufficient on its own to produce lasting change. There is a risk that psychoeducation may become overly didactic, focusing on delivering information rather than facilitating experiential learning and emotional processing.
Clients may intellectually understand their condition yet still struggle to apply this knowledge in real-life situations. For example, knowing that anxiety is harmless does not automatically eliminate anxious responses. Therefore, psychoeducation must be integrated with experiential techniques such as behavioral practice, emotional exploration, and skills training.
Balancing “knowing” with “doing” is critical. Psychoeducation should serve as a foundation that supports, rather than replaces, other therapeutic processes.
6. Variability in Cognitive Abilities and Learning Styles: Clients differ widely in their cognitive capacities, literacy levels, and preferred learning styles. Some may benefit from verbal explanations, while others may respond better to visual, experiential, or interactive methods. Individuals with cognitive impairments, learning difficulties, or severe mental health conditions may require simplified or adapted senses.
Failure to accommodate these differences can limit the accessibility and effectiveness of psychoeducation. Clinicians should use a variety of teaching methods (such as diagrams, metaphors, role-plays, and written materials) to ensure that information is understood and retained. Checking for understanding and inviting questions are also essential components of effective delivery.
7. Potential for Misinterpretation or Misuse of Information: Another challenge lies in the possibility that clients may misinterpret or selectively apply psychoeducational information. For example, learning about the biological basis of a disorder might lead some individuals to adopt a deterministic view, believing that change is not possible. Others may use diagnostic labels to over-identify with their condition, limiting their sense of identity beyond the illness.
To address this, clinicians must provide balanced and nuanced explanations, emphasizing both the biological and psychological aspects of mental health as well as the potential for change and recovery. Encouraging critical thinking and ongoing dialogue can help prevent rigid or maladaptive interpretations.
8. Engagement and Motivation Barriers: Not all clients are equally motivated to engage with psychoeducational content. Some may view it as irrelevant, overly academic, or disconnected from their immediate concerns. Others may resist information that challenges deeply held beliefs or requires behavioral change.
Enhancing engagement requires making psychoeducation interactive, relatable, and directly applicable to the client’s life. Linking information to personal goals, using real-life examples, and incorporating collaborative discussions can increase relevance and motivation. Integrating psychoeducation with motivational approaches can also help address ambivalence and resistance.
9. Ethical and Professional Considerations: Psychoeducation must be delivered within ethical and professional boundaries. Providing inaccurate, outdated, or overly generalized information can mislead clients and undermine trust. Clinicians have a responsibility to ensure that the content is evidence-based and communicated in a way that is honest and transparent.
Additionally, psychoeducation should respect client autonomy. While it aims to inform and guide, it should not be used to impose decisions or pressure clients into specific treatments. Shared decision-making and informed consent are essential components of ethical practice.
In conclusion, psychoeducation has emerged as a vital component of therapeutic practice, offering a powerful means of empowering clients through knowledge, insight, and skill development. Its applications span a wide range of mental health conditions and therapeutic settings, from individual therapy to family and group interventions. Evidence consistently demonstrates its effectiveness in enhancing treatment adherence, reducing relapse, and improving overall outcomes. More prominently, psychoeducation reflects a broader shift in mental health care toward collaboration and client empowerment. By recognizing clients as active participants in their recovery, psychoeducation not only informs but transforms the therapeutic process. As research continues to evolve, integrating psychoeducation with emerging approaches such as neuroscience-informed care and mindfulness-based interventions will further strengthen its role in promoting sustainable mental health and well-being.
Frequently Asked Questions (FAQs):
What is psychoeducation in therapy?
Psychoeducation is a therapeutic approach that involves providing clients and their families with structured, evidence-based information about mental health conditions, treatment options, coping strategies, and recovery processes. It is not just about giving information; it also involves discussion, reflection, and skill-building to help clients actively manage their difficulties.
How is psychoeducation different from regular advice or counseling?
Unlike general advice, psychoeducation is grounded in scientific research and clinical practice. It focuses on helping clients understand the why behind their experiences, rather than simply telling them what to do. It is also collaborative, encouraging clients to connect the information to their own lives and participate actively in treatment.
Who can benefit from psychoeducation?
Psychoeducation is beneficial for a wide range of individuals, including those experiencing anxiety, depression, bipolar disorder, schizophrenia, addiction, and ADHD. It is also valuable for family members, caregivers, and even individuals without a diagnosed condition who want to improve their mental health awareness and coping skills.
Is psychoeducation used alone or with other therapies?
Psychoeducation can be used as a standalone intervention in some cases, but it is most commonly integrated with other therapeutic approaches such as cognitive-behavioral therapy (CBT), mindfulness-based therapies, and motivational interviewing. It enhances the effectiveness of these treatments by improving understanding and engagement.
How does psychoeducation help in recovery?
Psychoeducation supports recovery by increasing insight, reducing stigma, and teaching practical coping strategies. It helps clients recognize symptoms, understand triggers, and apply skills to manage their condition. This leads to better treatment adherence, reduced relapse risk, and improved overall functioning.
Can psychoeducation reduce relapse in mental health conditions?
Yes, psychoeducation is particularly effective in reducing relapse in chronic conditions such as bipolar disorder and schizophrenia. By teaching individuals to identify early warning signs and maintain treatment routines, it enables proactive management and prevents the escalation of symptoms.
Is psychoeducation suitable for children and adolescents?
Yes, psychoeducation can be adapted for children and adolescents using age-appropriate language and methods. It is especially useful in conditions like ADHD, where both the child and caregivers benefit from understanding the condition and learning behavioral management strategies.
What role do families play in psychoeducation?
Families play a crucial role, especially in conditions that require long-term management. Family psychoeducation helps relatives understand the condition, improve communication, and provide effective support. This often leads to better outcomes and a more supportive home environment.
Are there any limitations to psychoeducation?
While psychoeducation is highly beneficial, it has limitations. It may be less effective if it is too complex, not tailored to the individual, or delivered at the wrong time. Additionally, knowledge alone is not enough; clients must also apply what they learn through practice and behavioral change.
How can therapists make psychoeducation more effective?
Therapists can enhance effectiveness by tailoring information to the client’s needs, using simple and clear language, incorporating interactive methods (e.g., discussions, exercises), and linking information to real-life situations. Ensuring collaboration and checking for understanding are also key.
Does psychoeducation address stigma related to mental illness?
Yes, one of its important functions is reducing stigma. By explaining that mental health conditions have biological, psychological, and social causes, psychoeducation helps individuals move away from self-blame and societal misconceptions, fostering acceptance and openness.
How long does psychoeducation take in therapy?
Psychoeducation is not a one-time activity; it is an ongoing process integrated throughout therapy. It may begin in early sessions with basic information and continue as more advanced concepts and skills are introduced over time.
Can psychoeducation improve motivation for change?
Yes, psychoeducation enhances motivation by helping clients understand the consequences of their behaviors and the benefits of change. When combined with approaches like motivational interviewing, it can significantly increase readiness and commitment to treatment.
Is psychoeducation effective in group settings?
Absolutely, group psychoeducation is widely used and effective, particularly for anxiety and depression. It offers additional benefits such as peer support, shared experiences, and normalization, making it both impactful and cost-effective.
What is the ultimate goal of psychoeducation?
The ultimate goal of psychoeducation is to empower individuals with knowledge, skills, and confidence so they can take an active role in managing their mental health. It aims to transform clients from passive recipients of care into informed and capable participants in their recovery journey.
References:
- Anderson, C. M., Hogarty, G. E., & Reiss, D. J. (1980). Family treatment of adult schizophrenic patients: A psycho-educational approach. Schizophrenia Bulletin, 6(3), 490–505. https://doi.org/10.1093/schbul/6.3.490
- Chien, W. T., Cheng, H. Y., McMaster, T. W., Yip, A. L. K., & Wong, J. J. C. L. (2019). Effectiveness of a mindfulness-based psychoeducation group programme for early-stage schizophrenia: An 18-month randomized controlled trial. Schizophrenia Research, 212, 140–149. https://doi.org/10.1016/j.schres.2019.07.053
- Dolan, N., Simmonds‐Buckley, M., Kellett, S., Siddell, E., & Delgadillo, J. (2021). Effectiveness of stress control large group psychoeducation for anxiety and depression: Systematic review and meta-analysis. British Journal of Clinical Psychology, 60(3), 375–399. https://doi.org/10.1111/bjc.12288
- Ekhtiari, H., Rezapour, T., Aupperle, R. L., & Paulus, M. P. (2017). Neuroscience-informed psychoeducation for addiction medicine: A neurocognitive perspective. Progress in Brain Research, 239–264. https://doi.org/10.1016/bs.pbr.2017.08.013
- Hettema, J., Steele, J., & Miller, W. R. (2005). Motivational interviewing. Annual Review of Clinical Psychology, 1(1), 91–111. https://doi.org/10.1146/annurev.clinpsy.1.102803.143833
- Parikh, S. V., Zaretsky, A., Beaulieu, S., et al. (2012). A randomized controlled trial of psychoeducation or cognitive-behavioral therapy in bipolar disorder. The Journal of Clinical Psychiatry, 73(6), 803–810. https://doi.org/10.4088/jcp.11m07343
- Powell, L. A., Parker, J., Weighall, A., & Harpin, V. (2021). Psychoeducation intervention effectiveness to improve social skills in young people with ADHD: A meta-analysis. Journal of Attention Disorders, 26(3), 340–357. https://doi.org/10.1177/1087054721997553
- Swift, J. K., & Parkin, S. R. (2017). The client as the expert in psychotherapy: What clinicians and researchers can learn about treatment processes and outcomes from psychotherapy clients. Journal of Clinical Psychology, 73(11), 1486–1488. https://doi.org/10.1002/jclp.22528
- Unterecker, S. (2019). Compliance and psychoeducation. In NeuroPsychopharmacotherapy (pp. 1–9). https://doi.org/10.1007/978-3-319-56015-1_6-1
Meta Psychological Education focuses on the foundational, higher-order skills (meta-skills) that allow individuals to “learn how to learn,” manage their own cognitive processes, and adapt to new situations, often termed meta-learning. It bridges psychological research with practical application in learning and development.




{kind=link}